Resident: Roberts
Date: 4/2/10
Article title: Adverse events and outcomes of conscious sedation for pediatric patients; study of an oral sedation regimen
Author: Leelataweedwud, pattarawadee, et al.
Journal: Jada
Volume: 132 month: November
Year: 2001
Method and Materials:
In a five year retrospective study, the authors examined 195 records of conscious sedation performed in 111 healthy children aged 24 months to 48 months. The author analyzed age, sex, weight, methods of drug delivery, waiting time after administration, adverse events, and sedation outcomes. The sedation regimen used was a cocktail of chloral hydrate (50mg/kg), meperidine (1.5mg/kg), hydroxizine pamoate (25mg) and supplemental oxygen.
Results: All of the following categories were compared in a table to satisfactory sedations, unsatisfactory sedations, and aborted cases to find any correlations if possible. Satisfactory defined as treatment completed without difficulty. Unsatisfactory defined as completed with difficulty or treatment not completed – due to disruptive behavior. Aborted – not attempted.
Age S: 24-80 months ( avg. 48mo w/sd of 13), U: 27 - 66 months (avg. 44 +-11),
A: 33-84 months (avg. 46+- 15)
Sex S: (M -77 F - 64), U: (M-21 F-23), A: (M-2 F-8)
Weight in kg S: 11-34 (avg. 17 +-3), U: 10 – 20 (avg16+-2), A: 10-23 (avg16+-3)
methods of drug delivery according to pt compliance
- all meds drunk 174/195 S: 131 (75%), U: 36 (21%), A: 7 (4%)
- meds delivered by syringe 21/195 S: 10 (48%), U: 8 (38%), A: 3 (14%)
waiting time after administration in min. S: 30 – 115 (avg. 61+-11), U: 30-75 (avg. 58+-11),
A: 35-65 (avg. 49+-12)
treatment time duration in min. S: 65+-22, U: 64+-24, A: N/A
adverse events S: 6 (100%), U: 0 (0%), A: 0 (0%)
apnea - defined as no visual signs of breathing, no audible signs from a precordial stethoscope Out of the 195 cases reviewed, only one case was recorded.
vomiting – defined as vomiting after the administration of the drug and before discharge requirements are met. Only 1 case incident was recorded in the study
desaturation – defined as an Spo2 reading from a pulse oximeter that fell below below95% while the patient was quiet and still. Only one incident was recorded.
prolonged sedation – defined as prolonged sedation time after all dental treatment is finished in which more than 30 minutes or more of recovery time is necessary to achieve discharge criteria recommended by the AAPD’s guidelines. A total of 3 incidents were found.
Conclusions
The described regimen of Chloral hydrate, meperidine, hydroxizine, and supplemental oxygen yielded a 72% overall success rate, while 23 percent of cases were unsuccessful, and 5 percent were aborted. Compliance with taking the full amount of oral sedation and waiting time prior to treatment (of around 60 min) were the most important factors for predicting success. Age, sex, and duration of treatment seamed to be less reliable predictors for success. Only 3% of cases resulted in adverse events occurring.
Assessment: I thought the author did a great job of reviewing the history of OCS cases performed. Though the conclusion was simple and precise he also had a lot of good information covered throughout his article pertaining to these drugs and this regimen. So for those of you that are interested in reading more, I would say go for it.
Tuesday, March 30, 2010
Monday, March 29, 2010
Upper airway obstruction during midazolam/nitrous oxide sedation in children with enlarged tonsils
Dan Boboia 4/2/10 Lit. Review
Title: Upper airway obstruction during midazolam/nitrous oxide sedation in children with enlarged tonsils
Author: Litman et al
Main Purpose: To examine the incidence and severity of upper airway obstruction in children with enlarged tonsils during the inhalation of 50% N2O after premed. with oral versed.
Methods:
25 children presenting for tonsillectomy were used as the study population and 25 children presenting for other types of elective surgery were used as control. Following premed with Versed (0.5mg/kg) measurements were collected during a 3-minute control period followed by 3 min. of breathing 50% N2O with 50% O2. An anesthesiologist held a mask over the child’s mouth and nose without supporting the head and neck or attempting to maintain airway patency. Every 20 seconds the airway patency was graded as none, partial, or complete based on clinical signs and capnography. Clinical signs included chest rise, stridor, and feeling movement of the ventilation bag.
Results:
During 50% N2O inhalation 14 children in the tonsillectomy group and four in the control group demonstrated upper airway obstruction (UAO). One child in the tonsillectomy group developed hypoxemia (SpO2 = 72%). One child in the tonsil group developed complete UAO (50%).
Conclusion:
Children who receive sedation with oral Versed and 50% N2O may exhibit significant UAO, especially in the presence of enlarged tonsils. Presedation physical exams should evaluate the presence of tonsil size during examination of the mouth and airway.
Title: Upper airway obstruction during midazolam/nitrous oxide sedation in children with enlarged tonsils
Author: Litman et al
Main Purpose: To examine the incidence and severity of upper airway obstruction in children with enlarged tonsils during the inhalation of 50% N2O after premed. with oral versed.
Methods:
25 children presenting for tonsillectomy were used as the study population and 25 children presenting for other types of elective surgery were used as control. Following premed with Versed (0.5mg/kg) measurements were collected during a 3-minute control period followed by 3 min. of breathing 50% N2O with 50% O2. An anesthesiologist held a mask over the child’s mouth and nose without supporting the head and neck or attempting to maintain airway patency. Every 20 seconds the airway patency was graded as none, partial, or complete based on clinical signs and capnography. Clinical signs included chest rise, stridor, and feeling movement of the ventilation bag.
Results:
During 50% N2O inhalation 14 children in the tonsillectomy group and four in the control group demonstrated upper airway obstruction (UAO). One child in the tonsillectomy group developed hypoxemia (SpO2 = 72%). One child in the tonsil group developed complete UAO (50%).
Conclusion:
Children who receive sedation with oral Versed and 50% N2O may exhibit significant UAO, especially in the presence of enlarged tonsils. Presedation physical exams should evaluate the presence of tonsil size during examination of the mouth and airway.
Thursday, March 25, 2010
Prevention and Treatment of Overweight in Children and Adolescents
Resident: Roberts
Date: Mar 26, 2010
Article title: Prevention and Treatment of Overweight in Children and Adolescents
Journal: American Family Physician
Volume: 69, number 11 pages: 2591-2598
Year : 2004
Discussion:
Recent studies suggest that 15 percent of children/adolescents in America are at risk for being overweight and 15 percent of them are. The status for being “at risk for being overweight” is correlated with the BMI, this is given to patients when their BMI is between the 85th and 95th percentile. A child that is overweight must have a BMI that is above the 95 percentile. A number of studies have shown that adolescent obesity can lead to an increased mortaility, morbidity and have an effect on social and economic welfare in adulthood. The effectiveness on weight loss interventionin adolescents is not well studied or understood. However, most intervention programs attempt to apply a combination of four treatment strategies which are: 1) Caloric restriction, 2) lifestyle exercise, 3) Decrease in sedentary behavior, 4) pharmateuticals (only in severe cases). Physicians should monitor BMI for all adolescent patients and deliver treatment strategies when individual problems have been identified. There are 3 ways to manage these case scenarios.
· BMI is less than 85 percentile: pt is not overweight and physician should reinforce healthy behaviors and monitor BMI periodically
· BMI is between 85 – 94 percentile: pt is at risk for obesity and physician should initiate weight maintenance strategies until pt can outgrow “at risk status.” Weight loss program may be initiated if necessary as well.
· BMI is above 94 percentile: pt is overweight and weight loss program should be initiated
Patients who are at risk/ or overweight shouldhave support from educated family, friends, doctors and nutritionist when possible and follow up appts should be conducted until goals are met.
Assessment: As pediatric dentists, our role should be identifying unhealthy eating habits and encouraging patients to change centain behaviors thus aiding in this process.
Date: Mar 26, 2010
Article title: Prevention and Treatment of Overweight in Children and Adolescents
Journal: American Family Physician
Volume: 69, number 11 pages: 2591-2598
Year : 2004
Discussion:
Recent studies suggest that 15 percent of children/adolescents in America are at risk for being overweight and 15 percent of them are. The status for being “at risk for being overweight” is correlated with the BMI, this is given to patients when their BMI is between the 85th and 95th percentile. A child that is overweight must have a BMI that is above the 95 percentile. A number of studies have shown that adolescent obesity can lead to an increased mortaility, morbidity and have an effect on social and economic welfare in adulthood. The effectiveness on weight loss interventionin adolescents is not well studied or understood. However, most intervention programs attempt to apply a combination of four treatment strategies which are: 1) Caloric restriction, 2) lifestyle exercise, 3) Decrease in sedentary behavior, 4) pharmateuticals (only in severe cases). Physicians should monitor BMI for all adolescent patients and deliver treatment strategies when individual problems have been identified. There are 3 ways to manage these case scenarios.
· BMI is less than 85 percentile: pt is not overweight and physician should reinforce healthy behaviors and monitor BMI periodically
· BMI is between 85 – 94 percentile: pt is at risk for obesity and physician should initiate weight maintenance strategies until pt can outgrow “at risk status.” Weight loss program may be initiated if necessary as well.
· BMI is above 94 percentile: pt is overweight and weight loss program should be initiated
Patients who are at risk/ or overweight shouldhave support from educated family, friends, doctors and nutritionist when possible and follow up appts should be conducted until goals are met.
Assessment: As pediatric dentists, our role should be identifying unhealthy eating habits and encouraging patients to change centain behaviors thus aiding in this process.
GERD
Resident: Adam J. Bottrill
Date: 26MAR10
Region: Providence
Article title: GERD
Major topic: GERD
Minor topic(s): Erosion
Key points:
1. Define GERD. Chronic symptoms or mucosal damage produced by the abnormal reflux in the esophagus. This is commonly due to transient or permanent changes in the barrier between the esophagus and the stomach. This can be due to incompetence of the lower esophageal sphincter, transient lower esophageal sphincter relaxation, impaired expulsion of gastric reflux from the esophagus, or a hiatal hernia. Respiratory and laryngeal manifestations of GERD are commonly referred to as extra esophageal reflux disease (EERD).
A. GERD may be difficult to detect in infants and children. Symptoms may vary from typical adult symptoms. GERD in children may cause repeated vomiting, effortless spitting up, coughing, and other respiratory problems. Inconsolable crying, failure to gain adequate weight, refusing food, bad breath, and belching or burping are also common. Children may have one symptom or many — no single symptom is universal in all children with GERD.
B. Common symptoms of Pediatric Reflux
* Irritability and pain, sometimes screaming suddenly when asleep. Constant or sudden crying or “colic” like symptoms. Babies can be inconsolable especially when laid down flat.
* Poor sleep habits typically with arching their necks and back during or after feeding
* Excessive possetting or vomiting
* Frequent burping or frequent hiccups
* Excessive dribbling or running nose
* Swallowing problems, gagging and choking
* Frequent ear infections or sinus congestion
* Babies are often very gassy and extremely difficult to “burp” after feeds
* Refusing feeds or frequent feeds for comfort
* Night time coughing, extreme cases of acid reflux can cause apnea and respiratory problems such as asthma, bronchitis and pneumonia if stomach contents are inhaled.
* Bad breath – smelling acidy
* Rancid/acid smelling diapers with loose stool. Bowel movements can be very frequent or babies can be constipated.
2. How does GERD effect the dentition? GERD can effect the dentition through the process of erosion. Almost ALL children with GERD have dental erosions.
3. Can GERD play a role in ECC? It can, however the surfaces effected by GERD are often different than those effected by ECC… this is a disputed fact.
4. What is the medical management? Dietary modification, positional therapy, weight loss, avoid tight garments, Meds (proton pump inhibitors, H2 receptor blockers, antacids), surgery.
5. What is a Nissen fundoplication (w/ or w/out pyloroplasty)? In a fundoplication, the gastric fundus (upper part) of the stomach is wrapped, or plicated, around the lower end of the esophagus and stitched in place, reinforcing the closing function of the lower esophageal sphincter: Whenever the stomach contracts, it also closes off the esophagus instead of squeezing stomach acids into it. This prevents the reflux of gastric acid (in GERD). The esophageal hiatus is also narrowed down by sutures to prevent or treat concurrent hiatal hernia, in which the fundus slides up through the enlarged esophageal hiatus of the diaphragm. In a Nissen fundoplication, also called a complete fundoplication, the fundus is wrapped all the way 360 degrees around the esophagus. Pyloroplasty, a procedure often accompanying fundoplication, is the term that describes the widening of the pylorus. This procedure assists with gastric emptying.

Assessment: Yay GERD.
Date: 26MAR10
Region: Providence
Article title: GERD
Major topic: GERD
Minor topic(s): Erosion
Key points:
1. Define GERD. Chronic symptoms or mucosal damage produced by the abnormal reflux in the esophagus. This is commonly due to transient or permanent changes in the barrier between the esophagus and the stomach. This can be due to incompetence of the lower esophageal sphincter, transient lower esophageal sphincter relaxation, impaired expulsion of gastric reflux from the esophagus, or a hiatal hernia. Respiratory and laryngeal manifestations of GERD are commonly referred to as extra esophageal reflux disease (EERD).
A. GERD may be difficult to detect in infants and children. Symptoms may vary from typical adult symptoms. GERD in children may cause repeated vomiting, effortless spitting up, coughing, and other respiratory problems. Inconsolable crying, failure to gain adequate weight, refusing food, bad breath, and belching or burping are also common. Children may have one symptom or many — no single symptom is universal in all children with GERD.
B. Common symptoms of Pediatric Reflux
* Irritability and pain, sometimes screaming suddenly when asleep. Constant or sudden crying or “colic” like symptoms. Babies can be inconsolable especially when laid down flat.
* Poor sleep habits typically with arching their necks and back during or after feeding
* Excessive possetting or vomiting
* Frequent burping or frequent hiccups
* Excessive dribbling or running nose
* Swallowing problems, gagging and choking
* Frequent ear infections or sinus congestion
* Babies are often very gassy and extremely difficult to “burp” after feeds
* Refusing feeds or frequent feeds for comfort
* Night time coughing, extreme cases of acid reflux can cause apnea and respiratory problems such as asthma, bronchitis and pneumonia if stomach contents are inhaled.
* Bad breath – smelling acidy
* Rancid/acid smelling diapers with loose stool. Bowel movements can be very frequent or babies can be constipated.
2. How does GERD effect the dentition? GERD can effect the dentition through the process of erosion. Almost ALL children with GERD have dental erosions.
3. Can GERD play a role in ECC? It can, however the surfaces effected by GERD are often different than those effected by ECC… this is a disputed fact.
4. What is the medical management? Dietary modification, positional therapy, weight loss, avoid tight garments, Meds (proton pump inhibitors, H2 receptor blockers, antacids), surgery.
5. What is a Nissen fundoplication (w/ or w/out pyloroplasty)? In a fundoplication, the gastric fundus (upper part) of the stomach is wrapped, or plicated, around the lower end of the esophagus and stitched in place, reinforcing the closing function of the lower esophageal sphincter: Whenever the stomach contracts, it also closes off the esophagus instead of squeezing stomach acids into it. This prevents the reflux of gastric acid (in GERD). The esophageal hiatus is also narrowed down by sutures to prevent or treat concurrent hiatal hernia, in which the fundus slides up through the enlarged esophageal hiatus of the diaphragm. In a Nissen fundoplication, also called a complete fundoplication, the fundus is wrapped all the way 360 degrees around the esophagus. Pyloroplasty, a procedure often accompanying fundoplication, is the term that describes the widening of the pylorus. This procedure assists with gastric emptying.

Assessment: Yay GERD.
Dental Management of Children with Asthma
Title: Dental management of children with asthma
Authors: Jian Fu Zhu DDS, Humberto Hidalgo MD MS, Corbett Holmgren DDS MD
Journal: Pediatric Dentistry 18:5 1996
Summary: Asthma is a chronic airway disease characterized by both inflammation and broncho-constriction due to genetic and environmental factors. It affects approximately 5-10% of children and is the leading cause of pediatric hospitalization in the US. Symptoms of asthma include coughing, wheezing, chest tightness and dyspnea. Tachypnea, tachycardia, diaphoresis and labored breathing can occur when the bronchial constriction is more severe. Asthma is broken down into mild (wheezing fewer than 2 days per week, no nocturnal symptoms and relatively good exercise tolerance), moderate (wheezing 2-5 days per week with nocturnal symptoms and poor exercise tolerance) and severe (daily wheezing, exercise intolerance and frequent nocturnal symptoms. Bronchocontstriction is mainly due to a hyper-responsive bronchus in the presence of triggering agents due to normal inflammation.
The most common cause of asthma attack is allergen exposures, viral or mycoplasma respiratory tract infections, nonspecific airway irritants, tapering of medication and exercise particularly in cold weather. More severe asthma is found in children of parents who smoke. Emotional and psychological stress may also bring on attacks. Aspirin and other beta adrenergic blockers may precipitate attacks, epinephrine may be used for these.
The two main types of drugs used to combat asthma are anti inflammatory drugs and bronchodilators. Mild asthma is usually controlled with only a beta receptor agonist such as albuterol or terbutaline (typically 2 puffs every 4-6 hours prn symptoms). Cromolyn sodium and nedocromil sodium are anti inflammatory agents that prevent mast cell release of mediators and are used in moderate cases, but have little effect against acute attacks. Inhaled corticosteroids are effective anti-inflammatories recommended for use in children with moderate to severe asthma. Systemic prednisone is also considered for those with acute severe asthma.
Asthma attacks should be considered as a medical emergency whose initial treatment is typically with albuterol, either from an inhaler or a nebulizer once the dental treatment has been discontinued. Keep the airway open and administer oxygen. If there is no improvement or the patient is worsening, administer epinephrine and summon medical assistance
There is evidence of a link between asthma and increased caries incidence, likely due to the 20% decrease in whole and 35% in parotid saliva due to beta agonist effects. Decreased nasorespiratory function can lead to mouth breathing which has been linked to narrower and higher palates, greater facial heights and increased risk of posterior crossbite. Inhaled steroid therapy has been associated with adrenal suppression, dysphonia, dryness of mouth, oropharyngeal candidiasis and rarely, tongue enlargement.
Asthmatics have a higher correlation with psychological problems. High dose prednisone therapy may result in anxiety or depression. Inhaled albuterol has also ben linked to hand tremors. Parents of asthmatic children tend to have a higher anxiety level than parents of healthy children.
When treating an asthmatic patient, the dentist can estimate how well the disease is controlled by asking: the frequency of attakcs, type of medication used chronically and for acute attacks and the length of time the child was last seen emergently due to asthma. A wheezing or poorly controlled patient should be reappointed, and inhalant bronchodilators should be brought to every appointment. Hydroxyzine is antihistaminic and benzodiazepines which are anxiolytic are recommended as agents of conscious sedation. Barbiturates and narcotics should be avoided in children with asthma because they may stimulate histamine release. Nitrous oxide use in children with mild to moderate asthma can help prevent acute attacks, but should be avoided in children with severe asthma since it can be an airway irritant. Ketamine is safe for asthmatic patients but may pose problems for children with cardiopulmonary problems. When possible, children with asthma should be treated with pulse oximetry, EKG and BP cuff present, with intubation materials available.
Patients taking theophylline should not receive erythromycin and it has been recommended to not use LA with vasocontrictors due to its beta agonist nature and the presence of meta bisulfites which may be highly allergic. Asthmatic children are three times more likely to have post operative complications than healthy children. Children who have been on daily or alternate day glucocrticoid therapy may become adrenally suppressed during treatment and should receive double their normal dose the day of treatment. These are patients who have had 4 or more 4-5+ day courses or a continuous 10-14 day course of systemic GC for acute asthma within the previous year and those who have taken systemic GC within the last 30 days. It has been recommended that these patients take 60mg hydrocortisone 6-8 hours before and 1 hour before, although this is not agreed upon.
Authors: Jian Fu Zhu DDS, Humberto Hidalgo MD MS, Corbett Holmgren DDS MD
Journal: Pediatric Dentistry 18:5 1996
Summary: Asthma is a chronic airway disease characterized by both inflammation and broncho-constriction due to genetic and environmental factors. It affects approximately 5-10% of children and is the leading cause of pediatric hospitalization in the US. Symptoms of asthma include coughing, wheezing, chest tightness and dyspnea. Tachypnea, tachycardia, diaphoresis and labored breathing can occur when the bronchial constriction is more severe. Asthma is broken down into mild (wheezing fewer than 2 days per week, no nocturnal symptoms and relatively good exercise tolerance), moderate (wheezing 2-5 days per week with nocturnal symptoms and poor exercise tolerance) and severe (daily wheezing, exercise intolerance and frequent nocturnal symptoms. Bronchocontstriction is mainly due to a hyper-responsive bronchus in the presence of triggering agents due to normal inflammation.
The most common cause of asthma attack is allergen exposures, viral or mycoplasma respiratory tract infections, nonspecific airway irritants, tapering of medication and exercise particularly in cold weather. More severe asthma is found in children of parents who smoke. Emotional and psychological stress may also bring on attacks. Aspirin and other beta adrenergic blockers may precipitate attacks, epinephrine may be used for these.
The two main types of drugs used to combat asthma are anti inflammatory drugs and bronchodilators. Mild asthma is usually controlled with only a beta receptor agonist such as albuterol or terbutaline (typically 2 puffs every 4-6 hours prn symptoms). Cromolyn sodium and nedocromil sodium are anti inflammatory agents that prevent mast cell release of mediators and are used in moderate cases, but have little effect against acute attacks. Inhaled corticosteroids are effective anti-inflammatories recommended for use in children with moderate to severe asthma. Systemic prednisone is also considered for those with acute severe asthma.
Asthma attacks should be considered as a medical emergency whose initial treatment is typically with albuterol, either from an inhaler or a nebulizer once the dental treatment has been discontinued. Keep the airway open and administer oxygen. If there is no improvement or the patient is worsening, administer epinephrine and summon medical assistance
There is evidence of a link between asthma and increased caries incidence, likely due to the 20% decrease in whole and 35% in parotid saliva due to beta agonist effects. Decreased nasorespiratory function can lead to mouth breathing which has been linked to narrower and higher palates, greater facial heights and increased risk of posterior crossbite. Inhaled steroid therapy has been associated with adrenal suppression, dysphonia, dryness of mouth, oropharyngeal candidiasis and rarely, tongue enlargement.
Asthmatics have a higher correlation with psychological problems. High dose prednisone therapy may result in anxiety or depression. Inhaled albuterol has also ben linked to hand tremors. Parents of asthmatic children tend to have a higher anxiety level than parents of healthy children.
When treating an asthmatic patient, the dentist can estimate how well the disease is controlled by asking: the frequency of attakcs, type of medication used chronically and for acute attacks and the length of time the child was last seen emergently due to asthma. A wheezing or poorly controlled patient should be reappointed, and inhalant bronchodilators should be brought to every appointment. Hydroxyzine is antihistaminic and benzodiazepines which are anxiolytic are recommended as agents of conscious sedation. Barbiturates and narcotics should be avoided in children with asthma because they may stimulate histamine release. Nitrous oxide use in children with mild to moderate asthma can help prevent acute attacks, but should be avoided in children with severe asthma since it can be an airway irritant. Ketamine is safe for asthmatic patients but may pose problems for children with cardiopulmonary problems. When possible, children with asthma should be treated with pulse oximetry, EKG and BP cuff present, with intubation materials available.
Patients taking theophylline should not receive erythromycin and it has been recommended to not use LA with vasocontrictors due to its beta agonist nature and the presence of meta bisulfites which may be highly allergic. Asthmatic children are three times more likely to have post operative complications than healthy children. Children who have been on daily or alternate day glucocrticoid therapy may become adrenally suppressed during treatment and should receive double their normal dose the day of treatment. These are patients who have had 4 or more 4-5+ day courses or a continuous 10-14 day course of systemic GC for acute asthma within the previous year and those who have taken systemic GC within the last 30 days. It has been recommended that these patients take 60mg hydrocortisone 6-8 hours before and 1 hour before, although this is not agreed upon.
Friday, March 19, 2010
Medical history
Medical History
From the Handbook, it should have:
- allergies
- adverse drug reactions
- immunizations
- current meds with dosages
- recurrent headaches
- congenital birth defects
- seizures
- developmental delays
- behavioral/learning problems
- hx of blood transfusions
- hx of abnormal bleeding
- problems with
o heart
o kidney
o liver/GI
o endocrine system
o breathing/lungs
o hearing
o vision
- history of
o cancers, tumors, blood dyscrasias
o hospitalizations, surgeries, injuries
o bacterial/viral infections (???)
o name/address of physician
o date of last physical exam
o substance abuse
o STD
o Pregnancy
o Any other issues?
- Family/social history
Should be consulted and updated at every visit. A new signed med hx should be obtained at every recall visit.
Needs to be signed and dated by legal guardian, and signed by person reviewing.
Sinusitis in Children: Define the condition and management strategies.
Resident: Roberts
Date:3/19/10
Author: Jane Desforges
Journal: Currrent concepts
Volume:326 No. 5
pages: 319-323
Sinusitis in Children: Define the condition and management strategies.
The condition:
Upper respiratory tract infections are the most common clinical problem encountered by primary care doctors. It has been estimated that between 5 and 10 percent of upper respiratory tract infections in early childhood are complicated by acute sinusitis. The maxillary, anterior ethmoidal, and frontal sinuses drain into the middle meatus, wheras the posterior ethmoidal and sphenoidal sinuses drain into the superior meatus. The lacrimal duct drains into the inferior meatus. The maxillary sinus has an awkward position which impedes gravitational drainage and predisposes patients to viral upper respiratory infections. The ethmoidal sinus has a number of small air cells separated by thin layer of bone which serves as a conduit into the enthomoidal sinus. If the mucosal lining is inflamed even a little by a viral respiratory infection, then an obstruction is likely. The sphenoidal and frontal sinisuses are not commonly associated with isolated obstructions but rather involved with episodes of parasinusitis. In order to maintain normal physiologic functioning of the sinuses one must have: patency of the ostia, functioning of the ciliary apparatus, and good quality of the secretions.
Management:
Persistant symptoms that last more than 10 but do not show signs of improving in less than 30 days are signs of acute sinusitis. The nasal discharge may be of any quality(thick, thin, clear, mucoid), cough present during the day and worse at night. The child may present with bad breath. The child may have a evident upper respiratory infection. The most common pathogen is strep. Pneumoniae, which accounts for 30 to 40 percent of all cases. H. influenza are similar and account for 20 percent of cases. Antimicrobial agents are the most comprehensive coverage for children with acute sinusitis. Amoxicillin, erythromycin, and cefuroximine are common choices. Sinus aspiration can be done but only in cases that do not respond to multiple courses of antibiotics.
Assesment: Interesting article
Date:3/19/10
Author: Jane Desforges
Journal: Currrent concepts
Volume:326 No. 5
pages: 319-323
Sinusitis in Children: Define the condition and management strategies.
The condition:
Upper respiratory tract infections are the most common clinical problem encountered by primary care doctors. It has been estimated that between 5 and 10 percent of upper respiratory tract infections in early childhood are complicated by acute sinusitis. The maxillary, anterior ethmoidal, and frontal sinuses drain into the middle meatus, wheras the posterior ethmoidal and sphenoidal sinuses drain into the superior meatus. The lacrimal duct drains into the inferior meatus. The maxillary sinus has an awkward position which impedes gravitational drainage and predisposes patients to viral upper respiratory infections. The ethmoidal sinus has a number of small air cells separated by thin layer of bone which serves as a conduit into the enthomoidal sinus. If the mucosal lining is inflamed even a little by a viral respiratory infection, then an obstruction is likely. The sphenoidal and frontal sinisuses are not commonly associated with isolated obstructions but rather involved with episodes of parasinusitis. In order to maintain normal physiologic functioning of the sinuses one must have: patency of the ostia, functioning of the ciliary apparatus, and good quality of the secretions.
Management:
Persistant symptoms that last more than 10 but do not show signs of improving in less than 30 days are signs of acute sinusitis. The nasal discharge may be of any quality(thick, thin, clear, mucoid), cough present during the day and worse at night. The child may present with bad breath. The child may have a evident upper respiratory infection. The most common pathogen is strep. Pneumoniae, which accounts for 30 to 40 percent of all cases. H. influenza are similar and account for 20 percent of cases. Antimicrobial agents are the most comprehensive coverage for children with acute sinusitis. Amoxicillin, erythromycin, and cefuroximine are common choices. Sinus aspiration can be done but only in cases that do not respond to multiple courses of antibiotics.
Assesment: Interesting article
Thursday, March 18, 2010
Physical Appearances of Children 3/19/10
Physical Appearances of Children
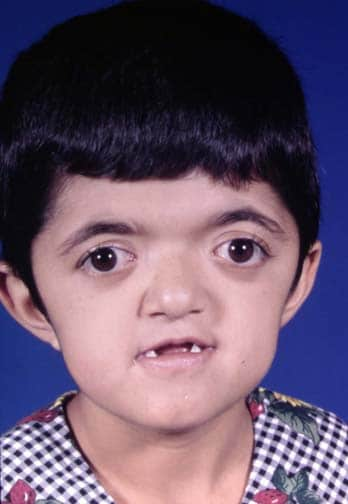
Head and Neck Features
Frontal Bossing
-Acromegaly
-Basal cell nevus syndrome
-Congenital syphilis
-Cleidocranial dysostosis
-Crouzon syndrome
-Hurler syndrome
-Pfeiffer syndrome
-Rubinstein-Taybi syndrome
-Russell-Silver syndrome (Russell-Silver dwarf)

Mutliple Frenae
-Orofacial digital Syn
-Thurston Syn
Hypertelorism
-Crouzon syndrome
-Apert syndrome
-Pfeiffer syndrome
-Saethre-Chotzen syndrome

Bifid Uvula,Tongue
-Associated with submucosa cleft
- Loey's Dietz Syndrome (LDS) and can involve some congenital heart problems, particularly aortic aneuyrsm

Flat Filtrum
-Fetal alcohol Syndrome
-Downs
-Hajdu-Cheney Syndrome
-cri du chat

Hair Color/Texture
http://dermatlas.med.jhmi.edu/derm/result.cfm?Diagnosis=-612507952
Cafe Au Lait Spots
- neurofibromatosis
-McCune-Albright syndrome.
-Von Hippel – Lindau disease
-Fanconi anemia
-Tuberous sclerosis
-Silver-Russell dwarfism
-Ataxia telangiectasia
-Bloom syndrome
-Basal cell nevus syndrome
-Gaucher disease
-Chédiak-Higashi syndrome
-Hunter syndrome
-Marfan's syndrome
-Maffucci syndrome
-McCune-Albright syndrome
-Peutz-Jeghers syndrome
-Multiple endocrine neoplasia type 2

Hemangiomas
-vascular formations
-Kasabach-Merritt syndrome



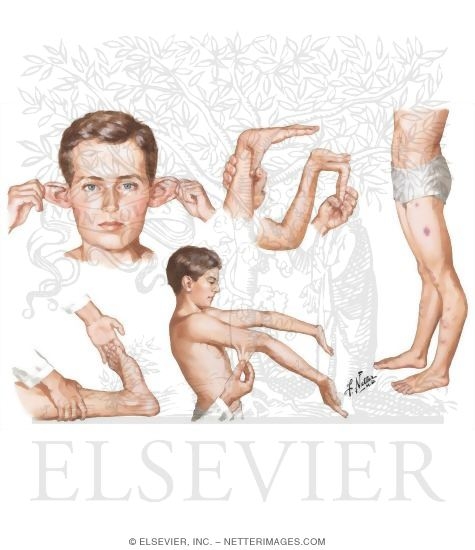
Digits and Extremities
Clubbing
-Chronic lung conditions
-Bronchiectasis
-Cystic fibrosis
-Lung abscess
-Lung cancer
-Pulmonary fibrosis
-Congenital heart disease (cyanotic type)
-Tetralogy of Fallot
-Total anomalous venous return
-Transposition of the great vessels
-Tricuspid atresia
-Truncus arteriosus
-Digestive system diseases
-Celiac disease
-Cirrhosis
-Crohn's disease and ulcerative colitis
-Graves disease or hyperthyroidism
-Dysentery
-Other types of cancer, including liver, gastrointestinal, Hodgkin's lymphoma
-Subacute endocarditis
-Tuberculosis of the intestines

Pitting Edema
-Acute glomerulonephritis
-Burns, including sunburn
-Chronic kidney disease
-Heart failure
-Liver failure from cirrhosis
-Nephrotic syndrome
-Poor nutrition
-Pregnancy
-Thyroid disease
-Too little albumin in the blood (hypoalbuminemia)
-Too much salt or sodium
Use of certain drugs, including
-Androgenic and anabolic steroids
-Calcium channel blockers
-Certain blood pressure medicines
-Corticosteroids such as prednisone
-Diabetes medicines called thiazolidinediones
-Estrogen
-Nonsteroidal anti-inflammatory drugs (NSAIDs)

Hyperkeratosis
-Hyperkeratosis is thickening of the stratum corneum, often associated with a qualitative abnormality of the keratin. Can be caused by Vit. A Def.
-Sacrlet fever
-Actinic keratosis

Polydactyly
-Dandy-Walker syndrome
-Pfieffer syndrome
-Familial polydactyly
-Carpenter syndrome
-Trisomy chromosome 13
-Short rib polydactyly syndrome
-Ellis-van Creveld syndrome
-Michel-Gruber syndrome


SYndactyly
- Acrosyndactyly;
- Delta Phalanx;
- Poland's syndrome:
- hypoplasia of hand and simple syndactyly of fingers on the same
side as the absent pectoral muscles (and other chest wall muscles);
- Apert's Syndrome:
- when all digits are joined, as is common in spoon hand of Apert's
syndrome (acrocephalosyndactyly), it is important to release
border digits-thumb and small finger-first;
- remaining 3 joined fingers can be managed by removing middle digit,
thus creating a three-fingered hand with a thumb and sufficient
skin for closure;
- Chromosomal Syndromes:
- trisomy of 13, 18, or 21;
- deletion of short arm of chromsome 5;
- Craniofacial Syndromes:
- Aglossia adactylia
- Mobius Syndrome
- Oculomandibulofacial syndrome


Head and Neck Features
Frontal Bossing
-Acromegaly
-Basal cell nevus syndrome
-Congenital syphilis
-Cleidocranial dysostosis
-Crouzon syndrome
-Hurler syndrome
-Pfeiffer syndrome
-Rubinstein-Taybi syndrome
-Russell-Silver syndrome (Russell-Silver dwarf)

Mutliple Frenae
-Orofacial digital Syn
-Thurston Syn
Hypertelorism
-Crouzon syndrome
-Apert syndrome
-Pfeiffer syndrome
-Saethre-Chotzen syndrome
Bifid Uvula,Tongue
-Associated with submucosa cleft
- Loey's Dietz Syndrome (LDS) and can involve some congenital heart problems, particularly aortic aneuyrsm

Flat Filtrum
-Fetal alcohol Syndrome
-Downs
-Hajdu-Cheney Syndrome
-cri du chat

Hair Color/Texture
http://dermatlas.med.jhmi.edu/derm/result.cfm?Diagnosis=-612507952
Cafe Au Lait Spots
- neurofibromatosis
-McCune-Albright syndrome.
-Von Hippel – Lindau disease
-Fanconi anemia
-Tuberous sclerosis
-Silver-Russell dwarfism
-Ataxia telangiectasia
-Bloom syndrome
-Basal cell nevus syndrome
-Gaucher disease
-Chédiak-Higashi syndrome
-Hunter syndrome
-Marfan's syndrome
-Maffucci syndrome
-McCune-Albright syndrome
-Peutz-Jeghers syndrome
-Multiple endocrine neoplasia type 2

Hemangiomas
-vascular formations
-Kasabach-Merritt syndrome



Digits and Extremities
Clubbing
-Chronic lung conditions
-Bronchiectasis
-Cystic fibrosis
-Lung abscess
-Lung cancer
-Pulmonary fibrosis
-Congenital heart disease (cyanotic type)
-Tetralogy of Fallot
-Total anomalous venous return
-Transposition of the great vessels
-Tricuspid atresia
-Truncus arteriosus
-Digestive system diseases
-Celiac disease
-Cirrhosis
-Crohn's disease and ulcerative colitis
-Graves disease or hyperthyroidism
-Dysentery
-Other types of cancer, including liver, gastrointestinal, Hodgkin's lymphoma
-Subacute endocarditis
-Tuberculosis of the intestines

Pitting Edema
-Acute glomerulonephritis
-Burns, including sunburn
-Chronic kidney disease
-Heart failure
-Liver failure from cirrhosis
-Nephrotic syndrome
-Poor nutrition
-Pregnancy
-Thyroid disease
-Too little albumin in the blood (hypoalbuminemia)
-Too much salt or sodium
Use of certain drugs, including
-Androgenic and anabolic steroids
-Calcium channel blockers
-Certain blood pressure medicines
-Corticosteroids such as prednisone
-Diabetes medicines called thiazolidinediones
-Estrogen
-Nonsteroidal anti-inflammatory drugs (NSAIDs)

Hyperkeratosis
-Hyperkeratosis is thickening of the stratum corneum, often associated with a qualitative abnormality of the keratin. Can be caused by Vit. A Def.
-Sacrlet fever
-Actinic keratosis

Polydactyly
-Dandy-Walker syndrome
-Pfieffer syndrome
-Familial polydactyly
-Carpenter syndrome
-Trisomy chromosome 13
-Short rib polydactyly syndrome
-Ellis-van Creveld syndrome
-Michel-Gruber syndrome


SYndactyly
- Acrosyndactyly;
- Delta Phalanx;
- Poland's syndrome:
- hypoplasia of hand and simple syndactyly of fingers on the same
side as the absent pectoral muscles (and other chest wall muscles);
- Apert's Syndrome:
- when all digits are joined, as is common in spoon hand of Apert's
syndrome (acrocephalosyndactyly), it is important to release
border digits-thumb and small finger-first;
- remaining 3 joined fingers can be managed by removing middle digit,
thus creating a three-fingered hand with a thumb and sufficient
skin for closure;
- Chromosomal Syndromes:
- trisomy of 13, 18, or 21;
- deletion of short arm of chromsome 5;
- Craniofacial Syndromes:
- Aglossia adactylia
- Mobius Syndrome
- Oculomandibulofacial syndrome


03/19/2010 Recognizing and managing the hypertensive child
Resident: Hencler
Date: 03/19/2010
Article title: Recognizing and managing the hypertensive child
Author: Flynn, MD, MS
Year: 2003
Major topic: Hypertension (HT)
Key points in the article discussion:
Awareness of childhood HT among the med community and the general public has increase. As a result, a greater number of children with HT have come to med attention. It is important to know the child’s height percentile b/f determining if BP is normal. Overall, most childhood HT is secondary to an underlying disorder, which in most cases, is renal disease. Today, obesity is a common cause of childhood HT. HT in children can also have a genetic basis although the role of genetic mutations in the pathophysiology of HT remains unknown. To obtain an accurate BP reading the bladder of the cuff should encircle 80%-100% of the circumference of the upper arm and it’s width should be 40%. The child should be seated quietly for at least 5 mins b/f BP reading and the arm should be supported at heart level. Once a child is found to have HP and thorough H & P, med and family hx should be conducted. Look for underlying symptoms of another disorder such as renal disease. B/c many children w/ HT have an otherwise normal physical exam, laboratory testing (full blood work up) is very important. Also assess the presence of hypertensive target-organ damage such as left vent hypertrophy or hypertensive retinopathy. Endocardiogrphy may also be required. Management is multifaceted including a comprehensive approach incorporating patient and family education, nonpharm measures, and anti-HT meds as well as monitoring med side effects and tx response. Encourage wieghtloss through diet modification and exercise. When prescribing anti-HT for children, the “stepped care” approach has been recommended. The dose of the initial agent chosen is increased until either, the BP is controlled, the max dose is reached, or side effects appear, then if BP not controlled a second agent is from a different class is added. Drug choice is up to doctor. Many pediatric authorities recommend against using diuretics as first line agents. The optimal BP goal of tx in a child w/ HT remains unknown. The lack of HT-related endpoints perhaps explains the lack of consensus on tx goals for HT children.
Summary:
Increased awareness of HT in children, coupled with an increase in risk factors for HT such as obesity, means that many more children will be found to have elevated BP.
Careful measurement of BP and evaluation of children with sustained HT should ID those for tx
Although outcome data for childhood HT does not yet exist, there has been a rapid increase in information regarding anti-HT drugs, making children easier to tx.
A combo of pharm and non-pharm measure will result in satisfactory control of childhood HT while allowing quality of life.
Assessment of article:
Useful information and very pertinent to anyone tx children.
Date: 03/19/2010
Article title: Recognizing and managing the hypertensive child
Author: Flynn, MD, MS
Year: 2003
Major topic: Hypertension (HT)
Key points in the article discussion:
Awareness of childhood HT among the med community and the general public has increase. As a result, a greater number of children with HT have come to med attention. It is important to know the child’s height percentile b/f determining if BP is normal. Overall, most childhood HT is secondary to an underlying disorder, which in most cases, is renal disease. Today, obesity is a common cause of childhood HT. HT in children can also have a genetic basis although the role of genetic mutations in the pathophysiology of HT remains unknown. To obtain an accurate BP reading the bladder of the cuff should encircle 80%-100% of the circumference of the upper arm and it’s width should be 40%. The child should be seated quietly for at least 5 mins b/f BP reading and the arm should be supported at heart level. Once a child is found to have HP and thorough H & P, med and family hx should be conducted. Look for underlying symptoms of another disorder such as renal disease. B/c many children w/ HT have an otherwise normal physical exam, laboratory testing (full blood work up) is very important. Also assess the presence of hypertensive target-organ damage such as left vent hypertrophy or hypertensive retinopathy. Endocardiogrphy may also be required. Management is multifaceted including a comprehensive approach incorporating patient and family education, nonpharm measures, and anti-HT meds as well as monitoring med side effects and tx response. Encourage wieghtloss through diet modification and exercise. When prescribing anti-HT for children, the “stepped care” approach has been recommended. The dose of the initial agent chosen is increased until either, the BP is controlled, the max dose is reached, or side effects appear, then if BP not controlled a second agent is from a different class is added. Drug choice is up to doctor. Many pediatric authorities recommend against using diuretics as first line agents. The optimal BP goal of tx in a child w/ HT remains unknown. The lack of HT-related endpoints perhaps explains the lack of consensus on tx goals for HT children.
Summary:
Increased awareness of HT in children, coupled with an increase in risk factors for HT such as obesity, means that many more children will be found to have elevated BP.
Careful measurement of BP and evaluation of children with sustained HT should ID those for tx
Although outcome data for childhood HT does not yet exist, there has been a rapid increase in information regarding anti-HT drugs, making children easier to tx.
A combo of pharm and non-pharm measure will result in satisfactory control of childhood HT while allowing quality of life.
Assessment of article:
Useful information and very pertinent to anyone tx children.
Role of the pediatric dentist in optimization of childhood immunization
Department of Pediatric Dentistry
Lutheran Medical Center
Date: 03/19/2010
Article title: Role of the pediatric dentist in optimization of childhood immunization
Author(s):Hicks, Flaitz
Journal: Pediatric Dentistry
Volume (number): 18:5
Month, Year: 1996
Major topic: Childhood immunization
Lutheran Medical Center
Date: 03/19/2010
Article title: Role of the pediatric dentist in optimization of childhood immunization
Author(s):Hicks, Flaitz
Journal: Pediatric Dentistry
Volume (number): 18:5
Month, Year: 1996
Major topic: Childhood immunization
Minor topics: Role of pediatric dentists beyond just dentistry
Type of Article: informative
Type of Article: informative
Main Purpose: To encourage pediatric dentists to play an active role in assisting children to obtain immunizations.
Overview of method of research: Professional opinion and presentation of statistics derived from other sources.
Overview of method of research: Professional opinion and presentation of statistics derived from other sources.
Findings:
Pediatric detists should keep immunization records of their patients and encourage parents under-immunized children to get immunized. Pediatric dentists can also provide proper referrals to assist in the process. Overall, this could diminish the spread of disease.
Key points/Summary :
Pediatric detists should keep immunization records of their patients and encourage parents under-immunized children to get immunized. Pediatric dentists can also provide proper referrals to assist in the process. Overall, this could diminish the spread of disease.
Key points/Summary :
- Many children are under-immunized.
- Parents often don’t know if their child has been properly immunized.
- Many children obtain immunizations from a variety of sources, making it harder to track.
- Dentists need to determine their own policies for treating under-immunized patients.
Assessment of article: A lot of text to make a very simple point, but this is good to keep in mind.
Scenario 1:
Autistic child whose parents think MMR caused autism and desire no future Immunizations. Does this matter:
If a parent believes that the MMR caused their child’s autism, then you aren’t going to change their mind. I would say “hey, your kid already has autism, so why not at least keep him from getting disease?”
From a public health standpoint it obviously does matter if the kid is immunized, but I personally could see why the parents would choose not to immunize.
Scenario 2:
trauma case with a dirty wound, no recored of a tetanus booster, what do you recommend?
Pt should be referred to PCP for tetanus booster per AAPD trauma guidelines.
Scenario 1:
Autistic child whose parents think MMR caused autism and desire no future Immunizations. Does this matter:
If a parent believes that the MMR caused their child’s autism, then you aren’t going to change their mind. I would say “hey, your kid already has autism, so why not at least keep him from getting disease?”
From a public health standpoint it obviously does matter if the kid is immunized, but I personally could see why the parents would choose not to immunize.
Scenario 2:
trauma case with a dirty wound, no recored of a tetanus booster, what do you recommend?
Pt should be referred to PCP for tetanus booster per AAPD trauma guidelines.
Wednesday, March 17, 2010
Hear Murmurs, Dan Boboia
1) Different types of murmurs?
Still's murmur - located at inferior aspect of lower left sternal border(LLSB), there is a systolic ejection sound, vibratory/musical quality; can be caused by subaortic stenosis, small VSD
- Pulmonary ejection - located at superior aspect of LLSB, ejection sound can be caused by atrial septal defect or pulmonary stenosis
- Venous hum- infraclavicular throughout the cardiac cycle (right side > left side), diminishes with jugular vein palpation or neck turning, common cause is PDA
- Supraclavicular arterial bruit; located above clavicles can be caused by aortic stenosis, bicuspid aortic valve
- Peripheral pulmonary stenosis; low-pitch with radiation to back and armpit can be cause by PDA, pulmonary stenosis
------------------------------------------------------------------------------------
Murmurs can be classified by seven different characteristics: timing, shape, location, radiation, intensity, pitch and quality.
· Timing refers to whether the murmur is a systolic or diastolic murmur.
· Shape refers to the intensity over time; murmurs can be crescendo, decrescendo or crescendo-decrescendo.
· Location refers to where the heart murmur is auscultated best. There are 6 places on the anterior chest to listen for heart murmurs; the first five out of six are adjacent to the sternum. Each of these locations roughly correspond to a specific part of the heart. The locations are: 2nd right intercostal space, 2nd - 5th left intercostal spaces, and 5th mid-clavicular intercostal space.
· Radiation refers to where the sound of the murmur radiates. The general rule of thumb is that the sound radiates in the direction of the blood flow.
· Intensity refers to the loudness of the murmur, and is graded on a scale from 0-6/6.
Grading of Murmurs Grade Description
· Grade 1 Very faint
· Grade 2 Soft
· Grade 3 Heard all over the precordium
· Grade 4 Loud, with palpable thrill (ie, a tremor or vibration felt on palpation)
· Grade 5 Very loud, with thrill. May be heard when stethoscope is partly off the chest.
· Grade 6 Very loud, with thrill. May be heard with stethoscope entirely off the chest.
· The pitch of a murmur is low, medium or high and is determined by whether it can be auscultated best with the bell or diaphragm of a stethoscope.
· Some examples of the quality of a murmur are: blowing, harsh, rumbling and musical.
-------------------------------------------------------------------------------------
2) Which murmurs require prophylaxis.
All murmurs associated with the conditions on Table 2 (Infective Endocarditis: Dental Implications and New Guidelines for Antibiotic Prophylaxis)
-------------------------------------------------------------------------------------
3) Acyanotic vs. Cyanotic Heart Defects
Acyanotic Types
· Left to Right Shunt Lesions – causing volume overload distal to the shunt with secondary congestive heart failure; symptoms: dyspnea, poor feeding, recurrent pneumonia, pulmonary congestion
· Obstructive Lesions – pulmonary stenosis, aortic stenosis, peripheral pulmonary stenosis, coarctation of the aorta; symptoms: limitation of exercise tolerance, chest pain or syncope, congestive heart failure and death if left untreated.
· Primary Pump Failure – dialated cardiomyopathy, myocarditis, anomalous origin of a coronary artery from the pulmonary artery
Cyanotic Congenital Heart Disease
1) Abnormal communication Proximal to Right-Sided Obstruction – right to left shunt when the right- and left sided pressures in the proximal chambers equalize (Tetrology of Fallot).
2) Abnormalities of Alignment Between Various Segments – D-transposition of the great arteries
-------------------------------------------------------------------------------------
4) Best way to communicate with a physician
Through a phone consult and ultimately a form of documentation that will end up in the patient's dental chart. If a pathological condition exists a cardiologist is often involved (usually a better resource then a primary care physician; more appropriate to obtain a consult from especially in cases of significant cardiac abnormality).
Still's murmur - located at inferior aspect of lower left sternal border(LLSB), there is a systolic ejection sound, vibratory/musical quality; can be caused by subaortic stenosis, small VSD
- Pulmonary ejection - located at superior aspect of LLSB, ejection sound can be caused by atrial septal defect or pulmonary stenosis
- Venous hum- infraclavicular throughout the cardiac cycle (right side > left side), diminishes with jugular vein palpation or neck turning, common cause is PDA
- Supraclavicular arterial bruit; located above clavicles can be caused by aortic stenosis, bicuspid aortic valve
- Peripheral pulmonary stenosis; low-pitch with radiation to back and armpit can be cause by PDA, pulmonary stenosis
------------------------------------------------------------------------------------
Murmurs can be classified by seven different characteristics: timing, shape, location, radiation, intensity, pitch and quality.
· Timing refers to whether the murmur is a systolic or diastolic murmur.
· Shape refers to the intensity over time; murmurs can be crescendo, decrescendo or crescendo-decrescendo.
· Location refers to where the heart murmur is auscultated best. There are 6 places on the anterior chest to listen for heart murmurs; the first five out of six are adjacent to the sternum. Each of these locations roughly correspond to a specific part of the heart. The locations are: 2nd right intercostal space, 2nd - 5th left intercostal spaces, and 5th mid-clavicular intercostal space.
· Radiation refers to where the sound of the murmur radiates. The general rule of thumb is that the sound radiates in the direction of the blood flow.
· Intensity refers to the loudness of the murmur, and is graded on a scale from 0-6/6.
Grading of Murmurs Grade Description
· Grade 1 Very faint
· Grade 2 Soft
· Grade 3 Heard all over the precordium
· Grade 4 Loud, with palpable thrill (ie, a tremor or vibration felt on palpation)
· Grade 5 Very loud, with thrill. May be heard when stethoscope is partly off the chest.
· Grade 6 Very loud, with thrill. May be heard with stethoscope entirely off the chest.
· The pitch of a murmur is low, medium or high and is determined by whether it can be auscultated best with the bell or diaphragm of a stethoscope.
· Some examples of the quality of a murmur are: blowing, harsh, rumbling and musical.
-------------------------------------------------------------------------------------
2) Which murmurs require prophylaxis.
All murmurs associated with the conditions on Table 2 (Infective Endocarditis: Dental Implications and New Guidelines for Antibiotic Prophylaxis)
-------------------------------------------------------------------------------------
3) Acyanotic vs. Cyanotic Heart Defects
Acyanotic Types
· Left to Right Shunt Lesions – causing volume overload distal to the shunt with secondary congestive heart failure; symptoms: dyspnea, poor feeding, recurrent pneumonia, pulmonary congestion
· Obstructive Lesions – pulmonary stenosis, aortic stenosis, peripheral pulmonary stenosis, coarctation of the aorta; symptoms: limitation of exercise tolerance, chest pain or syncope, congestive heart failure and death if left untreated.
· Primary Pump Failure – dialated cardiomyopathy, myocarditis, anomalous origin of a coronary artery from the pulmonary artery
Cyanotic Congenital Heart Disease
1) Abnormal communication Proximal to Right-Sided Obstruction – right to left shunt when the right- and left sided pressures in the proximal chambers equalize (Tetrology of Fallot).
2) Abnormalities of Alignment Between Various Segments – D-transposition of the great arteries
-------------------------------------------------------------------------------------
4) Best way to communicate with a physician
Through a phone consult and ultimately a form of documentation that will end up in the patient's dental chart. If a pathological condition exists a cardiologist is often involved (usually a better resource then a primary care physician; more appropriate to obtain a consult from especially in cases of significant cardiac abnormality).
Friday, March 12, 2010
Multiple developmental dental anomalies and hyper mobility type Ehlers-Danlos syndrome
Resident: Roberts
Date: 3/12/10
Article title: Multiple developmental dental anomalies and hyper mobility type Ehlers-Danlos syndrome
Author: Othman, Yassin
Journal: The Journal of Pediatric Dentistry
Year: 2006
Discussion:
Ehlers Danlos syndrome(EDS) is a relatively rare group of heritable connective tissue disorders with a clinical and genetic heterogeneity characterized mainly by articular hypermobility, skin extensibility, and tissue fragility. EDS is caused by disordered fibrillar collagen metabolism due to deficiency of collagen-processing enzymes, dominant-negative effects of mutant-chains, and haploinsufficiency. In this case report, a 15 year old, Jordanian boy was referred to a pediatric clinic for a general assessment of mandibular hypdontia. The family history revealed that he was eight out of ten siblings; and with the exception of a sister who had died of Burkett’s lymphoma at age 10, there was no history of illness or disease among his siblings. His parents appeared to be healthy and normal. The child was in the 3rd percentile for height, 50th percentile for weight. He presented with rather normal physiologic features other than delayed puberty, broad nasal bridge and generalized joint hyper mobility. His medical history presented with a heart murmur that expressed regurgitation, and a number of hormones that were deficient – (FSH), (LH), and free testosterone. Intraorally, he presented with seven teeth that did not erupt: the manibular incisors, mandibular left second premolar, and maxillary second molars. Three mandibular teeth were partially erupted: the right second premolar and second molar, and the left canine ectopically and partially erupting along the midline. Of the primary dentition the manidibular primary left canine was retained, and gave no history of tooth extraction or traumatic loss. The teeth were of normal color, size and form. The patient exhibited class III malocclusion. A panorex showed the absence of permanent mandibular incisors, and pulp stones in all of his permanent teeth. His molars had stunted roots, and his canines were dilacerated. His appeared to have generalized bone loss in the posterior areas of his mouth. None of his sibling showed any signs of dental anomalies.
Assessment: great article and interesting to read.
Date: 3/12/10
Article title: Multiple developmental dental anomalies and hyper mobility type Ehlers-Danlos syndrome
Author: Othman, Yassin
Journal: The Journal of Pediatric Dentistry
Year: 2006
Discussion:
Ehlers Danlos syndrome(EDS) is a relatively rare group of heritable connective tissue disorders with a clinical and genetic heterogeneity characterized mainly by articular hypermobility, skin extensibility, and tissue fragility. EDS is caused by disordered fibrillar collagen metabolism due to deficiency of collagen-processing enzymes, dominant-negative effects of mutant-chains, and haploinsufficiency. In this case report, a 15 year old, Jordanian boy was referred to a pediatric clinic for a general assessment of mandibular hypdontia. The family history revealed that he was eight out of ten siblings; and with the exception of a sister who had died of Burkett’s lymphoma at age 10, there was no history of illness or disease among his siblings. His parents appeared to be healthy and normal. The child was in the 3rd percentile for height, 50th percentile for weight. He presented with rather normal physiologic features other than delayed puberty, broad nasal bridge and generalized joint hyper mobility. His medical history presented with a heart murmur that expressed regurgitation, and a number of hormones that were deficient – (FSH), (LH), and free testosterone. Intraorally, he presented with seven teeth that did not erupt: the manibular incisors, mandibular left second premolar, and maxillary second molars. Three mandibular teeth were partially erupted: the right second premolar and second molar, and the left canine ectopically and partially erupting along the midline. Of the primary dentition the manidibular primary left canine was retained, and gave no history of tooth extraction or traumatic loss. The teeth were of normal color, size and form. The patient exhibited class III malocclusion. A panorex showed the absence of permanent mandibular incisors, and pulp stones in all of his permanent teeth. His molars had stunted roots, and his canines were dilacerated. His appeared to have generalized bone loss in the posterior areas of his mouth. None of his sibling showed any signs of dental anomalies.
Assessment: great article and interesting to read.
Thursday, March 11, 2010
Department of Pediatric Dentistry
Resident’s Name: Murphy Program: Lutheran Medical Center - Providence
Article title: Orthodontic Treatment Protocol of Ehlers Danlos Syndrome Type VI
Author(s): Arun, Tulin. Didem Nalbantgil, Krkmaz Sayinsu
Journal: Angle Orthodontist
Year. Volume (number). Page #’s: 2006, 76(1). 177-183
Major topic: Considerations for orthodontically treating a patient with Ehlers Danlos Syndrome(EDS).
Overview of method of research: A 17 year old male with EDS was treated orthodontically, and followed throughout treatment
Findings: EDS is characterized by abnormalities of CT leading to fragility of the skin and blood vessels, hyperextensibility, and hyermobility of joints. The patient in the report was class 3, extensive crowding, supernumerary teeth (one mesiodens), and bilateral anterior and posterior cross-bites. The initial treatment plan included surgery due to the severity of the class 3. However this was ruled out due to the increased risks of bleeding, poor healing, and the increased possibility of complication later on in treatment. The supernumerary tooth was extracted. A lower incisor was extracted after a wax setup was completed. Rapid palatal expansion had to be performed to obtain enough space and to fix the cross-bites. The maxillary incisors were flared for proper overbite/overjet. The case was finished in 34 months, and the patient was fit with permanent retention.
Because patients with EDS have poor healing, special care should be given to their oral hygiene and periodontal status. The patient was put on 3 month recall so he could be closely monitored. Also, because patients with EDS have hypermobility and usually a history of subluxing joints, special care should be given to the TMJ. It was ensured that the patient did not stay open for too long, or open too wide during appointments. A TMJ exam was completed every 6 months to ensure its health. Due to the fragility of CT in EDS patients, there can be increased mobility of teeth during treatment. This can stress the periodontal fibers, resulting in slow repair. Therefore, slow, light force was used throughout treatment to avoid any untoward effects.
Key points/Summary: When treating a patient with EDS remember….
1. There may be decreased wound healing and vascular fragility. Don’t do surgery unless you have to!
2. They are hyermobile, and often sublux joints. Don’t make them stay open for too long, or too wide.
3. Keep a close eye on their periodontium and STRESS OHI.
4. Hyermobility of teeth can be normal.
5. If you’re doing ortho, use light force.
Assessment of Article: Good review on what to keep in mind when treating a patient with EDS. Holla back.
Ehlers-Danlos syndrome identified from periodontal findings: case report
Resident: Adam J. Bottrill
Date: 11MAR10
Region: Providence
Article title: Ehlers-Danlos syndrome identified from periodontal findings: case report
Author(s): Bond, P et al.
Journal: Pediatric Dentostry
Page #s: pp. 212-213
Year: 1993, May/June
Major topic: Ehlers-Danlos
Minor topic(s): Periodontal disease
Type of Article: Case Report
Main Purpose: Case report on type VIII Ehlers-Danlos patient with periodontal findings.
Overview of method of research: Case research
Key points in the article discussion:
I. Ehlers-Danlos: connective tissue disorder characterized by fragile skin, skin hyperextensibility, joint hypermobility. Type VIII was 1st described in 1972.
A. Autosomal dominant, post-pubertal periodontal disease, pretibial scarring,
B. NO joint hypermobility or skin hyperextensibility
C. Typically significant amount of overlap between type VIII and type IV (which can be fatal)
II. Case of HW
A. 7 yo white female with NSMH, NSDH, no FH.
B. Presents with parents “concerned about the appearance of her teeth.
C. Severe generalized gingivitis, recession and exposed root surfaces.
D. Radiograph revealed 4-5mm bony pockets.
E. Heavy calculus and premature exfoliating teeth.
F. Systemic disease suspected. (prolonged bleeding time, peritibial bruising)
G. Referal was made: EDS type VIII was Dx.
III. Discussion
A. Rare condition
B. DDX: histiocytosis X, cyclic neutropenia, Papillon-Lefevre, hypophosphatasia, leukemia, vit D resistant rickets, leukocyte disorders, acrodynia …. AND … EDS type VIII.
C. Because of possibility of EDS type IV and it’s potentially fatal prognosis, must include the EDS’s in DDX.
Assessment of article: Simple. Short. To the point… Semper Vigilans!!!
Date: 11MAR10
Region: Providence
Article title: Ehlers-Danlos syndrome identified from periodontal findings: case report
Author(s): Bond, P et al.
Journal: Pediatric Dentostry
Page #s: pp. 212-213
Year: 1993, May/June
Major topic: Ehlers-Danlos
Minor topic(s): Periodontal disease
Type of Article: Case Report
Main Purpose: Case report on type VIII Ehlers-Danlos patient with periodontal findings.
Overview of method of research: Case research
Key points in the article discussion:
I. Ehlers-Danlos: connective tissue disorder characterized by fragile skin, skin hyperextensibility, joint hypermobility. Type VIII was 1st described in 1972.
A. Autosomal dominant, post-pubertal periodontal disease, pretibial scarring,
B. NO joint hypermobility or skin hyperextensibility
C. Typically significant amount of overlap between type VIII and type IV (which can be fatal)
II. Case of HW
A. 7 yo white female with NSMH, NSDH, no FH.
B. Presents with parents “concerned about the appearance of her teeth.
C. Severe generalized gingivitis, recession and exposed root surfaces.
D. Radiograph revealed 4-5mm bony pockets.
E. Heavy calculus and premature exfoliating teeth.
F. Systemic disease suspected. (prolonged bleeding time, peritibial bruising)
G. Referal was made: EDS type VIII was Dx.
III. Discussion
A. Rare condition
B. DDX: histiocytosis X, cyclic neutropenia, Papillon-Lefevre, hypophosphatasia, leukemia, vit D resistant rickets, leukocyte disorders, acrodynia …. AND … EDS type VIII.
C. Because of possibility of EDS type IV and it’s potentially fatal prognosis, must include the EDS’s in DDX.
Assessment of article: Simple. Short. To the point… Semper Vigilans!!!
Title: Epidermolysis bullosa
Authors: Heddie Sedano DDS and Robert J. Gorlin DDS MS
Journal: Oral Surgery Oral Medicine and Oral Pathology
Dates: May 1989
Topic: review of types and symptoms of EB
Summary:
Epidermolysis Bullosa Simplex: most frequently involved in sites of friction or trauma; altered nails in ~20% of cases; no scarring or pigmentation following healing. Often affects the hands, feet and neck. Most often found neonatally or in infants. Intraoral blisters are less severe than other forms of EB. Teeth are not affected.
EB Atrophicans Generalisata Gravis (Herlitz type): present within the first few hours of life and hemorrhagic vesicles are seen at the base of the fingernails. The face and scalp are also affected. Palms and soles are never affected. Fragile and hemorrhagic vesicles are found at the junction of hard and soft palates. Hypoplastic and pitted enamel leading to extensive caries principally in the molar teeth. Many die in the first few months, those who survive have syndactyly, anemia, growth retardation and nail dystrophy. Perioral and perinasal crusted and granular hemorrhagic lesions are pathognomonic in adult patients.
Dominant Dystrophic Form: Flat, pink scar producing bullae of the ankles, knees and hands. 20% of patients manifest oral bullae.
Scarring EB with Dermolytic Blisters: 4 different types with bullae usually manifesting at or shortly after birth, caused by pressure ad trauma. In infants, the occiput, the scapulas, elbows, fingers buttocks and feet are most affected. The bullae leave painful ulcers upon rupture. Keloidal scars often follow healing. Formation of clawhand and enclosure of the hand in a glovelike epidermal sac have been noted frequently. Dwarfism can be secondary to scarring in growth areas.Shrinkage of the conjunctiv aand keratitis with corneal opacity has also been noted. Hoarseness, aphonea and dysphagia may result due to bulla in the larynx. Hypoplastic enamel rapidly affected by dental caries, delayed eruption and frequent retention. Oral mucosal vesicles form soon after birth from the negative pressure from sucking. The lingual mucosa appears thick, gray and smooth. Repeated blistering may lead to limited opening and akyloglossia. Other related conditions are severe periodontal disease with alveolar bone resorption, atrophy of the maxilla with resultant relative mandibular prognathism, increased mandibular angle and oral carcinoma.
EB acquisita: blisters in areas of trauma; associated with amyloidosis, multiple myeloma, diabetes meelitus and IBD (may represent a GI cutaneous syndrome with an immune pathogenesis). Extensive dental caries, leading to complete loss of teeth has been noted in every patient with this condition.
EB non scarring atrophicans generalisata mitis: oral mucosal bulla,nodular excrescences on the palate and gingiva, some cases present with pitted enamel.
Assessment: Interesting but a lot of 'sometimes' and 'may lead to' implying.
Authors: Heddie Sedano DDS and Robert J. Gorlin DDS MS
Journal: Oral Surgery Oral Medicine and Oral Pathology
Dates: May 1989
Topic: review of types and symptoms of EB
Summary:
Epidermolysis Bullosa Simplex: most frequently involved in sites of friction or trauma; altered nails in ~20% of cases; no scarring or pigmentation following healing. Often affects the hands, feet and neck. Most often found neonatally or in infants. Intraoral blisters are less severe than other forms of EB. Teeth are not affected.
EB Atrophicans Generalisata Gravis (Herlitz type): present within the first few hours of life and hemorrhagic vesicles are seen at the base of the fingernails. The face and scalp are also affected. Palms and soles are never affected. Fragile and hemorrhagic vesicles are found at the junction of hard and soft palates. Hypoplastic and pitted enamel leading to extensive caries principally in the molar teeth. Many die in the first few months, those who survive have syndactyly, anemia, growth retardation and nail dystrophy. Perioral and perinasal crusted and granular hemorrhagic lesions are pathognomonic in adult patients.
Dominant Dystrophic Form: Flat, pink scar producing bullae of the ankles, knees and hands. 20% of patients manifest oral bullae.
Scarring EB with Dermolytic Blisters: 4 different types with bullae usually manifesting at or shortly after birth, caused by pressure ad trauma. In infants, the occiput, the scapulas, elbows, fingers buttocks and feet are most affected. The bullae leave painful ulcers upon rupture. Keloidal scars often follow healing. Formation of clawhand and enclosure of the hand in a glovelike epidermal sac have been noted frequently. Dwarfism can be secondary to scarring in growth areas.Shrinkage of the conjunctiv aand keratitis with corneal opacity has also been noted. Hoarseness, aphonea and dysphagia may result due to bulla in the larynx. Hypoplastic enamel rapidly affected by dental caries, delayed eruption and frequent retention. Oral mucosal vesicles form soon after birth from the negative pressure from sucking. The lingual mucosa appears thick, gray and smooth. Repeated blistering may lead to limited opening and akyloglossia. Other related conditions are severe periodontal disease with alveolar bone resorption, atrophy of the maxilla with resultant relative mandibular prognathism, increased mandibular angle and oral carcinoma.
EB acquisita: blisters in areas of trauma; associated with amyloidosis, multiple myeloma, diabetes meelitus and IBD (may represent a GI cutaneous syndrome with an immune pathogenesis). Extensive dental caries, leading to complete loss of teeth has been noted in every patient with this condition.
EB non scarring atrophicans generalisata mitis: oral mucosal bulla,nodular excrescences on the palate and gingiva, some cases present with pitted enamel.
Assessment: Interesting but a lot of 'sometimes' and 'may lead to' implying.
Tuesday, March 9, 2010
03/12/2010 Oral manifestations of Ehlers-Danlos syndrome Type VII: histological examination of a primary tooth
Resident: J. Hencler
Date: 03/12/2010
Article title: Oral manifestations of Ehlers-Danlos syndrome Type VII: histological examination of a primary tooth
Author(s): Ooshima ET AL.
Journal: Pediatric Dentistry: April/May, 1990 ~ Vol. 12, No. 2, Pg 102-106
Major topic: Ehlers-Danlos syndrome Type VII and associated dental histology
Type of Article: Case Presentation
Main Purpose: Describe a patient with E-D syndrome Type VII and define the associated dental manifestations.
Background:
E-D syndrome is a heterogeneous grp of hereditable disorders of connective tissue. Clinical feature common to all E-D syndromes include skin hyperextensibility, joint hypermobility, and skin fragility. At least 11 types are known. Oral manifestations include fragility of oral mucosa w/ delayed healing, microdontia, short or malformed roots, large pulp stones and calcification of the pulp, bleeding after tooth brushing, and PD.
Patient:
2 year old Japanese girl with E-D syndrome Type VII dx at 3 months. Physical exam at birth revealed dislocation of right hip, swan neck deformities of the fingers, joint hypermobility, skin fragility, and skin hyperextensibility. Her unaffected parents were first cousins. At 3 year old she had severe genus valgus making it impossible for her to walk.
Materials and Methods:
Measurements of MD/BL dimensions of the primary teeth were made on study models and compared to a mean value. EXTed teeth and pulp tissue were examined under microscope with various dye treatments.
Key points in the article discussion:
E-D syndrome Type VII is caused by the deficiency of procollagen peptidase in collagen biogenesis. In this patient presence of marked joint hypermobility, congenital dislocation of hip, and various skin symptoms at birth were consistent w/ dx of E-D syndrome Type VII. Dental finding in our pt were yellow teeth, microdontia, and bleeding after tooth brushing. The MD/BL dimensions of the pts teeth fell below the mean crown size of primary teeth in normal Japanese children. Pulp stones and pulp obliteration, the principle dental manifestations described in previous reports of E-D syndrome were not observed in our patient on radiographic examination. H & E stained sections of the pulp showed a few minute calcified bodies, etiology unknown. The incidence of pulp calcification appears to increase with age. Therefore it is difficult to conclude that the pulp calcification in the present case is one of the principal oral manifestations of Type VII E-D syndrome. There were several inclusions that appeared fistulous in the dentin of this patient. The inclusions were surrounded by an inner highly calcified region and surrounded by an outer poorly calcified region. The staining revealed lesser amounts of collagen or the presence of non-collagenous substances. A laminated calcified matrix w/ fewer dentinal tubules and multiple cell inclusions also was found in the dentin adjacent to the pulp in the tooth of this patient. The tooth had pulpal inflammation, which may have contributed to the devel of the laminated calcified matrix. The extent of the laminated calcified matrix was unusually thick when compared histologically to tertiary dentin of carious incisors in normal children. These findings may support that the dentin matrix has formed rapidly and elements in the pulp are incorporated into the dentin. However, the odontoblast function appears to be deficient in the production of collagen w/in the dentin matrix. The collagen in the pulp tissue in this E-D syndrome patient showed a wavy pattern, which was different from normal pulp tissue characterized by a network structure.
Summary of conclusions:
Most of the findings in this patient reflect the deficiency in collagen biosynthesis of E-D syndrome Type VII. Other dental manifestations such as PD, poor wound healing after EXT, and malformed roots of deciduous teeth were not observed in this patient.
Assessment of article:
Article was ok. All E-D syndrome patients will not present with every characteristic symptom while symptom severity may vary greatly in different patients. It is important to know the cardinal features of any syndrome so it will be recognized and the appropriate treatment approach can be determined.
Date: 03/12/2010
Article title: Oral manifestations of Ehlers-Danlos syndrome Type VII: histological examination of a primary tooth
Author(s): Ooshima ET AL.
Journal: Pediatric Dentistry: April/May, 1990 ~ Vol. 12, No. 2, Pg 102-106
Major topic: Ehlers-Danlos syndrome Type VII and associated dental histology
Type of Article: Case Presentation
Main Purpose: Describe a patient with E-D syndrome Type VII and define the associated dental manifestations.
Background:
E-D syndrome is a heterogeneous grp of hereditable disorders of connective tissue. Clinical feature common to all E-D syndromes include skin hyperextensibility, joint hypermobility, and skin fragility. At least 11 types are known. Oral manifestations include fragility of oral mucosa w/ delayed healing, microdontia, short or malformed roots, large pulp stones and calcification of the pulp, bleeding after tooth brushing, and PD.
Patient:
2 year old Japanese girl with E-D syndrome Type VII dx at 3 months. Physical exam at birth revealed dislocation of right hip, swan neck deformities of the fingers, joint hypermobility, skin fragility, and skin hyperextensibility. Her unaffected parents were first cousins. At 3 year old she had severe genus valgus making it impossible for her to walk.
Materials and Methods:
Measurements of MD/BL dimensions of the primary teeth were made on study models and compared to a mean value. EXTed teeth and pulp tissue were examined under microscope with various dye treatments.
Key points in the article discussion:
E-D syndrome Type VII is caused by the deficiency of procollagen peptidase in collagen biogenesis. In this patient presence of marked joint hypermobility, congenital dislocation of hip, and various skin symptoms at birth were consistent w/ dx of E-D syndrome Type VII. Dental finding in our pt were yellow teeth, microdontia, and bleeding after tooth brushing. The MD/BL dimensions of the pts teeth fell below the mean crown size of primary teeth in normal Japanese children. Pulp stones and pulp obliteration, the principle dental manifestations described in previous reports of E-D syndrome were not observed in our patient on radiographic examination. H & E stained sections of the pulp showed a few minute calcified bodies, etiology unknown. The incidence of pulp calcification appears to increase with age. Therefore it is difficult to conclude that the pulp calcification in the present case is one of the principal oral manifestations of Type VII E-D syndrome. There were several inclusions that appeared fistulous in the dentin of this patient. The inclusions were surrounded by an inner highly calcified region and surrounded by an outer poorly calcified region. The staining revealed lesser amounts of collagen or the presence of non-collagenous substances. A laminated calcified matrix w/ fewer dentinal tubules and multiple cell inclusions also was found in the dentin adjacent to the pulp in the tooth of this patient. The tooth had pulpal inflammation, which may have contributed to the devel of the laminated calcified matrix. The extent of the laminated calcified matrix was unusually thick when compared histologically to tertiary dentin of carious incisors in normal children. These findings may support that the dentin matrix has formed rapidly and elements in the pulp are incorporated into the dentin. However, the odontoblast function appears to be deficient in the production of collagen w/in the dentin matrix. The collagen in the pulp tissue in this E-D syndrome patient showed a wavy pattern, which was different from normal pulp tissue characterized by a network structure.
Summary of conclusions:
Most of the findings in this patient reflect the deficiency in collagen biosynthesis of E-D syndrome Type VII. Other dental manifestations such as PD, poor wound healing after EXT, and malformed roots of deciduous teeth were not observed in this patient.
Assessment of article:
Article was ok. All E-D syndrome patients will not present with every characteristic symptom while symptom severity may vary greatly in different patients. It is important to know the cardinal features of any syndrome so it will be recognized and the appropriate treatment approach can be determined.
Friday, March 5, 2010
EB - two case reports
Resident’s Name: Joanne Lewis Date: March 5, 2010
Article title: Epidermolysis bullosa: dental and anesthetic management of two cases
Author(s): J. Tim Wright, DDS, MS
Journal: Oral Surgery, February 1984, Volume 57, Number 2
Type of Article: case report
Main Purpose: to present the dental and anesthetic management of two severely affected EB patients.
Overview: Two siblings were diagnosed as having recessive epidermolysis bullosa atrophicans-gravis Herlitz; severe enamel hypoplasia with typical cutaneous, esophageal, and ocular lesions was seen in both cases. Both children required dental rehabilitation under general anesthesia. Special care was taken in the surgical management of the cases to prevent nosocomial infections or minor tissue trauma that might precipitate the formation of bullae. The special precautions were:
- synthetic sheepskin bedding was used on all carts, beds, and the operating table.
- patient’s arm was wrapped in guaze before placement of the blood pressure cuff.
- orotracheal intubation was used; the tubing, laryngoscope blade, and perioral area was lubricated with 1%hydrocortisone cream.
- moist guaze packs were place on one side of the orotracheal tube.
- prior to extubation, the anesthesiologist used an endoscope to check for bullae.
Dental treatment consisted of stainless steel crown and extractions.
Key points/Summary: Patients with EB often require early and extensive dental treatment – this dental treatment is most safely accomplished in the operating room using special precautions.
Assessment of article: interesting.
Thursday, March 4, 2010
Use of endosseous implants in a 3-year-old child with ectodermal dysplasia: case report and 5-year follow up
Resident: J. Hencler
Date: 03/05/2010
Article title:
Use of endosseous implants in a 3-year-old child with ectodermal dysplasia: case report and 5-year follow up
Author(s): Albert D. Guckes, DDS, MSD George R. McCarthy, DDS Jaime Brahim, DDS, MS
Journal: Pediatric Dentistry-19: 4, 1997
Major topic: Ectodermal dysplasia
Type of Article: Case Report
Main Purpose:
Present a case report of implant placement in a 3yo w/ ectodermal dysplasia, subsequent prostho tx, and 5 yr follow-up.
Background:
Ectodermal dysplasia represents a grp of inherited disorders characterized by defects in tissue that are derived from ectoderm.
Case:
3 yo white male dx w/ Christ-Siemens-Touraine ectodermal dysplasia. 4 mandibular and 2 maxillary implants were placed (stage 1 complete). Max/Mand bone augmentation with hydroxyapatite (HA) was completed. Clinical exam was consistent w/ dx of hypohidrotic ecto dysplasia. 2 max tooth buds observed. Implants healed normal, child scheduled for stage 2 uncovering of implants and placement of mand healing abutments. Maxillary right implant was removed due to mobility. Max left implant was covered b/c it alone could not contribute to prosthesis support. Max conventional complete denture and mand over-denture were fabricated and adjusted/remade over 5 yrs as needed to accommodate eruption of 2 max teeth and overall growth.
Follow-up:
Mand implants in function 4 yrs. Relative position w/in ant mand unchanged as growth occurs in the rami and condyles. Some resorption of HA noted radiographically after 5 yrs. Relative position of unloaded single max implant has not moved w/ the downward and forward growth of the maxilla but is positioned in close proximity to the nasal floor. This implant will require close monitoring, as the ultimate position is uncertain.
Key points in the article discussion:
This case confirms that implants placed int the ant mand wil move w/ the mand as growth occurs in the condyles and rami. Mand rotation that occurs w/ growth has not caused problems relative to implant angulation and prosthetic occl plane. The change in implant position of the max implant as the mand grows downward is not unexpected and may be a significant complication and may require removal. While the magnitude of the change in position of the max implant may not be typical, it provides a cautionary note regaeding implant placement in the growing maxilla. The most important issue raised by this case is if and when tx of a young child w/ implants is indicated and prudent. There is little research identifying any physiologic benefits of placing implants in children. The theoretical possibility exists that significant edentulism in a growing child adversely affects craniofacial growth. While the lit supports the concept that craniofacial devel is adversely affects in ecto dyplasia children, the exact mechanism by which the growth is affected is unclear. The most obvious effect of ecto dyplasia is lack of alveolar bone in areas of anodontia. At present there is no evidence from clinical trials to indicate that implant placement in young children has a positive effect on craniofacial growth and devel.
Summary of conclusions:
This case provides a good opportunity to follow the consequences of placing oral implants in a very young patient. Psychological benefits may be associated w/ using implant to support an oral prosthesis in the mandible of a teenage child with many missing teeth. However, clinical research has not demonstrated compelling reasons to place implants in pre-teenage children.
Assessment of article:
Very interesting article. Implant placement in the growing child will require multi-specialty extensive tx planning. I feel that ultimately it should be the parent’s decision once they are fully informed of prognosis and tx requirements including ongoing maintenance to accommodate for future growth.
Date: 03/05/2010
Article title:
Use of endosseous implants in a 3-year-old child with ectodermal dysplasia: case report and 5-year follow up
Author(s): Albert D. Guckes, DDS, MSD George R. McCarthy, DDS Jaime Brahim, DDS, MS
Journal: Pediatric Dentistry-19: 4, 1997
Major topic: Ectodermal dysplasia
Type of Article: Case Report
Main Purpose:
Present a case report of implant placement in a 3yo w/ ectodermal dysplasia, subsequent prostho tx, and 5 yr follow-up.
Background:
Ectodermal dysplasia represents a grp of inherited disorders characterized by defects in tissue that are derived from ectoderm.
Case:
3 yo white male dx w/ Christ-Siemens-Touraine ectodermal dysplasia. 4 mandibular and 2 maxillary implants were placed (stage 1 complete). Max/Mand bone augmentation with hydroxyapatite (HA) was completed. Clinical exam was consistent w/ dx of hypohidrotic ecto dysplasia. 2 max tooth buds observed. Implants healed normal, child scheduled for stage 2 uncovering of implants and placement of mand healing abutments. Maxillary right implant was removed due to mobility. Max left implant was covered b/c it alone could not contribute to prosthesis support. Max conventional complete denture and mand over-denture were fabricated and adjusted/remade over 5 yrs as needed to accommodate eruption of 2 max teeth and overall growth.
Follow-up:
Mand implants in function 4 yrs. Relative position w/in ant mand unchanged as growth occurs in the rami and condyles. Some resorption of HA noted radiographically after 5 yrs. Relative position of unloaded single max implant has not moved w/ the downward and forward growth of the maxilla but is positioned in close proximity to the nasal floor. This implant will require close monitoring, as the ultimate position is uncertain.
Key points in the article discussion:
This case confirms that implants placed int the ant mand wil move w/ the mand as growth occurs in the condyles and rami. Mand rotation that occurs w/ growth has not caused problems relative to implant angulation and prosthetic occl plane. The change in implant position of the max implant as the mand grows downward is not unexpected and may be a significant complication and may require removal. While the magnitude of the change in position of the max implant may not be typical, it provides a cautionary note regaeding implant placement in the growing maxilla. The most important issue raised by this case is if and when tx of a young child w/ implants is indicated and prudent. There is little research identifying any physiologic benefits of placing implants in children. The theoretical possibility exists that significant edentulism in a growing child adversely affects craniofacial growth. While the lit supports the concept that craniofacial devel is adversely affects in ecto dyplasia children, the exact mechanism by which the growth is affected is unclear. The most obvious effect of ecto dyplasia is lack of alveolar bone in areas of anodontia. At present there is no evidence from clinical trials to indicate that implant placement in young children has a positive effect on craniofacial growth and devel.
Summary of conclusions:
This case provides a good opportunity to follow the consequences of placing oral implants in a very young patient. Psychological benefits may be associated w/ using implant to support an oral prosthesis in the mandible of a teenage child with many missing teeth. However, clinical research has not demonstrated compelling reasons to place implants in pre-teenage children.
Assessment of article:
Very interesting article. Implant placement in the growing child will require multi-specialty extensive tx planning. I feel that ultimately it should be the parent’s decision once they are fully informed of prognosis and tx requirements including ongoing maintenance to accommodate for future growth.
Ehlers Danlos (Great Video)
Since my article was forthcoming I decided to post this super sweet video about my topic instead. We may not have time to watch it all, but we should at least watch a few minutes.
Anodontia with hypohidrotic ectodermal dysplasia in a young female: a case report
Resident: Roberts
Date: 3/5/10
Article title: Anodontia with hypohidrotic ectodermal dysplasia in a young female: a case report
Journal: Pediatric Dentistry
Volume: 22:1 pages: 49 – 52
Year: 2000
Discussion:
Anodontia is a rare condition, especially in females. It has been associated with the most severe forms of Ectodermal dysplasia - most commonly hypohidrotic E.D. Anodontia of the primary dentition can be diagnosed radiographically at birth, and of the permanent dentition by age 4. People with anodontia appear to have a senile facial appearance due to lack of teeth, and underdevelopment of the alveolar ridges. Since 1950 there have been many cases of extreme oligodontia or near anodontia reported, but very few cases of true anodontia (17 total). All cases of anodontia reported were associated with ectodermal dysplasia and occurred predominantly in males. In instances of anodontia of the permanent dentition only, it was found to be reported equally in both sexes. In all cases oral mucosa was normal and alveolar ridges were underdeveloped. Removable dentures are treatment of choice until implant supported prosthesis can be fabricated.
Assessment: An easy reader, I liked it.
Date: 3/5/10
Article title: Anodontia with hypohidrotic ectodermal dysplasia in a young female: a case report
Journal: Pediatric Dentistry
Volume: 22:1 pages: 49 – 52
Year: 2000
Discussion:
Anodontia is a rare condition, especially in females. It has been associated with the most severe forms of Ectodermal dysplasia - most commonly hypohidrotic E.D. Anodontia of the primary dentition can be diagnosed radiographically at birth, and of the permanent dentition by age 4. People with anodontia appear to have a senile facial appearance due to lack of teeth, and underdevelopment of the alveolar ridges. Since 1950 there have been many cases of extreme oligodontia or near anodontia reported, but very few cases of true anodontia (17 total). All cases of anodontia reported were associated with ectodermal dysplasia and occurred predominantly in males. In instances of anodontia of the permanent dentition only, it was found to be reported equally in both sexes. In all cases oral mucosa was normal and alveolar ridges were underdeveloped. Removable dentures are treatment of choice until implant supported prosthesis can be fabricated.
Assessment: An easy reader, I liked it.
Ectodermal Dysplasia
Resident: Adam J. Bottrill
Date: 05MAR10
Region: Providence
Article title: Ectodermal Dysplasia
Author(s): Wright, T. et al
Journal: ?
Page #s: pp. 17211724
Year: ?
Major topic: Ectodermal Dysplasia
Minor topic(s): N/A
Type of Article: Topic Summary
Main Purpose: Describe the different clinical characteristics of Ectodermal Dysplasia (ED)
Overview of method of research: Summary
Key points in the article discussion:
A. General
1. Includes all conditions having a developmental defect that embryologically affects the ectoderm.
2. Over 120 conditions classifiable as ED’s.
3. More recent definitions of ED include any one of the following: hypotrichosis, hypodontia, onychodysplasia, anhydrosis … PLUS ectodermal involvement.
4. Most types remain a purely clinical diagnosis… not yet molecularly characterized.
5. Other non-ectoderm structures may be involved: limbs, bones, palate, neuro, organs, repro.
6. Hair 90%, skin 85%, teeth 80%, nails 75%, face 72%
7. No FH, and often hard to diagnose… VERY few are localized to specific DNA and inheritance.
a. female carriers often have tooth involvement.
8. Most treatment is only preventative or palliative… there is no cure.
9. Dental implants are often treatment of choice as early as during teenage yrs.


Assessment of article: Keep it simple stupid.
Date: 05MAR10
Region: Providence
Article title: Ectodermal Dysplasia
Author(s): Wright, T. et al
Journal: ?
Page #s: pp. 17211724
Year: ?
Major topic: Ectodermal Dysplasia
Minor topic(s): N/A
Type of Article: Topic Summary
Main Purpose: Describe the different clinical characteristics of Ectodermal Dysplasia (ED)
Overview of method of research: Summary
Key points in the article discussion:
A. General
1. Includes all conditions having a developmental defect that embryologically affects the ectoderm.
2. Over 120 conditions classifiable as ED’s.
3. More recent definitions of ED include any one of the following: hypotrichosis, hypodontia, onychodysplasia, anhydrosis … PLUS ectodermal involvement.
4. Most types remain a purely clinical diagnosis… not yet molecularly characterized.
5. Other non-ectoderm structures may be involved: limbs, bones, palate, neuro, organs, repro.
6. Hair 90%, skin 85%, teeth 80%, nails 75%, face 72%
7. No FH, and often hard to diagnose… VERY few are localized to specific DNA and inheritance.
a. female carriers often have tooth involvement.
8. Most treatment is only preventative or palliative… there is no cure.
9. Dental implants are often treatment of choice as early as during teenage yrs.


Assessment of article: Keep it simple stupid.
Pattern of permanent teeth present in individuals with ectodermal dysplasia and severe hypodontia suggests treatment with dental implants 3/5/10
Department of Pediatric Dentistry
Resident’s Name: Murphy Program:Lutheran Medical Center - Providence
Article title: Pattern of permanent teeth present in individuals with ectodermal dysplasia and severe hypodontia suggests treatment with dental implants
Author(s): Gucker DDS, Albert, Michale Roberts DDS, George McCarthy DDS.
Journal: American Academy of Pediatric Dentistry
Year. Volume (number). Page #’s: 1998. 20:4. 278-280
Major topic: Ectodermal Dyplasia and it’s effects on teeth
Minor topic(s): Treatment options
Main Purpose: To assess the pattern of permanent teeth present in a self selected sample of patients with ectodermal dysplasia(ED) presenting for treatment with dental implants.
Overview of method of research: Panoramic radiographs of 17 female and 35 make patients were examined independently by two investigators to determine the permanent teeth present.
Findings: ED is an inherited disorder in which at least two structures derived from the ectoderm are abnormal. Oral findings of ED can include anodontia, hypodontia, and lack of ridge development. Hypodontia occurs in more than 80% of cases. Studies found that males show more symptoms of missing teeth than females. Physical signs can involve the sweat glands, scalp, hair, nails, skin pigment, and abnormal/underdevelopment of craniofacial structures. The two major types of ED are hypohidrotic, in which sweat glands are absent (most severe, sensitivity to heat, temperature), and hidrotic, in which sweat glands are normal.
The permanent teeth most likely to be present in patients with ED are listed below, starting with the most likely.
1. Maxillary Central Incisor 42%
2. Maxillary 1st molar 41%
3. Mandibular 1st molar 39%
4. Maxillary Canines 22%
5. Mandibular 2nd molars 17%
6. Maxillary 2nd premolars 15%
7. Mandibular premolars 12%
Mandibular anterior teeth were least likely to be present. Considerable research has shown the efficacy of rehabilitating a completely or partially edentulous mandible using implant supported prosthesis. Success rates are in the 90 percentile in adolescents and over 97% in adults(older than 17).
Key points/Summary: Bottom line, if a patient of yours has ED, with hypo/anodontia, implants should be considered as a treatment option. It’s definitive, accepted, proven success and could change a patients quality of life.
Assessment of Article: Money. SO money it doesn’t even know it.


http://images.google.com/imgres?imgurl=http://www.penchasdentistry.com/galleries/18/normal/blake.jpg&imgrefurl=http://www.penchasdentistry.com/gallery_images.html%3Fid%3D18&usg=__vZ7sD2H6VduEvtUdJwa-KyEdFCk=&h=448&w=297&sz=24&hl=en&start=15&sig2=AwkDrlGkklnkUiUBiUTSeQ&um=1&itbs=1&tbnid=6gNZIHlMqi9hQM:&tbnh=127&tbnw=84&prev=/images%3Fq%3Dectodermal%2Bdysplasia%26um%3D1%26hl%3Den%26sa%3DN%26rlz%3D1T4DMUS_enUS317US253%26tbs%3Disch:1&ei=lxiQS8byI8SW-gbRiaAn
Resident’s Name: Murphy Program:Lutheran Medical Center - Providence
Article title: Pattern of permanent teeth present in individuals with ectodermal dysplasia and severe hypodontia suggests treatment with dental implants
Author(s): Gucker DDS, Albert, Michale Roberts DDS, George McCarthy DDS.
Journal: American Academy of Pediatric Dentistry
Year. Volume (number). Page #’s: 1998. 20:4. 278-280
Major topic: Ectodermal Dyplasia and it’s effects on teeth
Minor topic(s): Treatment options
Main Purpose: To assess the pattern of permanent teeth present in a self selected sample of patients with ectodermal dysplasia(ED) presenting for treatment with dental implants.
Overview of method of research: Panoramic radiographs of 17 female and 35 make patients were examined independently by two investigators to determine the permanent teeth present.
Findings: ED is an inherited disorder in which at least two structures derived from the ectoderm are abnormal. Oral findings of ED can include anodontia, hypodontia, and lack of ridge development. Hypodontia occurs in more than 80% of cases. Studies found that males show more symptoms of missing teeth than females. Physical signs can involve the sweat glands, scalp, hair, nails, skin pigment, and abnormal/underdevelopment of craniofacial structures. The two major types of ED are hypohidrotic, in which sweat glands are absent (most severe, sensitivity to heat, temperature), and hidrotic, in which sweat glands are normal.
The permanent teeth most likely to be present in patients with ED are listed below, starting with the most likely.
1. Maxillary Central Incisor 42%
2. Maxillary 1st molar 41%
3. Mandibular 1st molar 39%
4. Maxillary Canines 22%
5. Mandibular 2nd molars 17%
6. Maxillary 2nd premolars 15%
7. Mandibular premolars 12%
Mandibular anterior teeth were least likely to be present. Considerable research has shown the efficacy of rehabilitating a completely or partially edentulous mandible using implant supported prosthesis. Success rates are in the 90 percentile in adolescents and over 97% in adults(older than 17).
Key points/Summary: Bottom line, if a patient of yours has ED, with hypo/anodontia, implants should be considered as a treatment option. It’s definitive, accepted, proven success and could change a patients quality of life.
Assessment of Article: Money. SO money it doesn’t even know it.

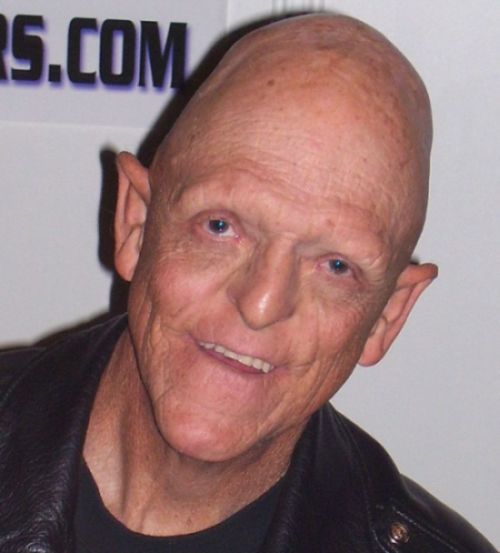
http://images.google.com/imgres?imgurl=http://www.penchasdentistry.com/galleries/18/normal/blake.jpg&imgrefurl=http://www.penchasdentistry.com/gallery_images.html%3Fid%3D18&usg=__vZ7sD2H6VduEvtUdJwa-KyEdFCk=&h=448&w=297&sz=24&hl=en&start=15&sig2=AwkDrlGkklnkUiUBiUTSeQ&um=1&itbs=1&tbnid=6gNZIHlMqi9hQM:&tbnh=127&tbnw=84&prev=/images%3Fq%3Dectodermal%2Bdysplasia%26um%3D1%26hl%3Den%26sa%3DN%26rlz%3D1T4DMUS_enUS317US253%26tbs%3Disch:1&ei=lxiQS8byI8SW-gbRiaAn
Hereditary epidermolysis bullosa:oral manifestations and dental management
Dan Boboia 3/5/10 Lit. Review
Title: Hereditary epidermolysis bullosa:oral manifestations and dental management
Author: Wright et al
Type of Article: Review
Summary:
Epidermolysis (EB) feature blister formation with tissue separation occuring at variable depths in the skin and under the mucosa (depending on the specific EB type). Oral involvement can occur. Although oral tissue fragility and blistering is common in all EB types, oral debilitation secondary to scarring is primarily limited to the recessive dystrophic EB subtypes. With junctional EB you often see generalized enamel hypoplasia. Rampant caries is associated with generalized recessive dystrophic EB. Intervention and prevention strategies targeting the dental effects of EB is often helpful in reducing the negative oral consequences associated with this disease. Patients with mild forms of EB are treated the same as those without the disorder. When using local anesthesia, injections should be deep and slow in order to prevent tissue distortion (which may cause mechanical tissue separation and blistering-nerve blocks are preferred). Apply only compressive forces rather then traction or other shear forces to oral tissues, these could induce tissue separation. Make certain to lubricate patient lips. Care must be taken with general anesthesia as to not induce airway obstruction secondary to blister formation. Generalized enamel hypoplasia, characteristic of junctional EB, is best managed with stainless steel crowns. Most individuals with EB can tolerate orthodontic therapy with minor design modifications to reduce soft tissue irritation. Small dental arches and collapsed dental arches do predispose these patients to significant crowding. Serial extractions can often benefit these patients. Fluoride rinses, Peridex rinses, soft-bristled toothbrushes with small heads may all help with caries control.
Assessment: Good review of oral management in these patients
Title: Hereditary epidermolysis bullosa:oral manifestations and dental management
Author: Wright et al
Type of Article: Review
Summary:
Epidermolysis (EB) feature blister formation with tissue separation occuring at variable depths in the skin and under the mucosa (depending on the specific EB type). Oral involvement can occur. Although oral tissue fragility and blistering is common in all EB types, oral debilitation secondary to scarring is primarily limited to the recessive dystrophic EB subtypes. With junctional EB you often see generalized enamel hypoplasia. Rampant caries is associated with generalized recessive dystrophic EB. Intervention and prevention strategies targeting the dental effects of EB is often helpful in reducing the negative oral consequences associated with this disease. Patients with mild forms of EB are treated the same as those without the disorder. When using local anesthesia, injections should be deep and slow in order to prevent tissue distortion (which may cause mechanical tissue separation and blistering-nerve blocks are preferred). Apply only compressive forces rather then traction or other shear forces to oral tissues, these could induce tissue separation. Make certain to lubricate patient lips. Care must be taken with general anesthesia as to not induce airway obstruction secondary to blister formation. Generalized enamel hypoplasia, characteristic of junctional EB, is best managed with stainless steel crowns. Most individuals with EB can tolerate orthodontic therapy with minor design modifications to reduce soft tissue irritation. Small dental arches and collapsed dental arches do predispose these patients to significant crowding. Serial extractions can often benefit these patients. Fluoride rinses, Peridex rinses, soft-bristled toothbrushes with small heads may all help with caries control.
Assessment: Good review of oral management in these patients
Subscribe to:
Comments (Atom)